Seborrheic Dermatitis

General Information
Seborrheic Dermatitis is a disease that causes flaking of the skin. Commonly called in adolescents and adults “dandruff.” In babies, it is known as “cradle cap.” It is aggravated by changes in humidity, changes in seasons, trauma (e.g., scratching), or emotional stress. Varying from mild dandruff to exfoliate erythroderma. Seborrheic dermatitis may worsen in patients that have Parkinson disease or AIDS. Distribution follows the oily and hair-bearing areas of the head and the neck, such as the scalp, the forehead, the eyebrows, the lash line, the nasolabial folds, the beard, and the postauricular skin. Dandruff can be treated with shampoos used twice a week that contain salicylic acid, the prescription selenium sulfide, or zinc pyrithione. Shampoos with coal tar may be used three times a week. If the shampoo alone does not help, a healthcare provider may prescribe a steroid lotion to be used once or twice daily, in addition to the shampoo. Steroid lotions may be used with seborrheic dermatitis of the skin creases in adolescents and adults. Seborrheic dermatitis of the scalp (cradle cap) in babies is treated with products that are not as strong as those used in adults are. Treatment for cradle cap should start with a mild, nonmedicated baby shampoo and brushing the baby’s scalp with a soft brush. If a nonmedicated shampoo does not work, your healthcare provider may prescribe a shampoo that contains tar or a shampoo that contains 2% ketoconazole may be prescribed. Seborrheic dermatitis of the skin creases in babies can be treated with gentle steroid lotions or creams.
Epidemiology
3-5% worldwide, slightly worse in males than in females
Etiology
Stress, fatigue, weather extremes, oily skin and infrequent shampooing or skin cleaning
Pathogenesis
Malassezia organisms (lipophilic yeast) are probably not the cause but are a cofactor linked to a T-cell depression, increased sebum levels, and an activation of the alternative complement pathway
Clinical
Appearance varies from mild, patchy scaling to widespread, thick, adherent crusts.
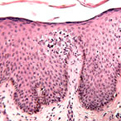
Histology
Hyperkeratosis, acanthosis, accentuated rete ridges, focal spoingiosis, and parakeratosis are characteristic.
Bibliography
1. “Seborrheic Dermatitis” (Online) May 2007. http://familydoctor.org/online/famdocen/home/common/skin/disorders/157.html (visited: March 15, 2008) 2. “Seborrheic Dermatitis” (Online). March 2007. http://www.emedicine.com/derm/topic396.htm (visited: March 15, 2008)
Download PDF
![]() Seborrheic Dermatitis
Seborrheic Dermatitis